The no-show problem is equally concrete. Peer-reviewed research published in PMC found that 67,000 no-shows can cost a healthcare system roughly $7 million, and a single vascular lab running a 12% no-show rate faced $89,107 in annual gross revenue loss. Reducing that rate to 5% would recover over $50,000.
Conversational AI voice agents now handle inbound booking requests, outbound reminders, and real-time rescheduling around the clock — in a way that IVR menus and patient portals were never built to do. This guide covers how the technology works, what providers concretely gain from it, and the compliance and deployment questions that matter most when evaluating a solution.
Key Takeaways
- No-shows and scheduling friction cost providers measurable revenue — automated AI reminders cut no-show rates by up to 40%
- Conversational AI understands natural speech — no phone menus, no scripted prompts
- AI agents run 24/7 with no hold queues, handling inbound booking and outbound reminders simultaneously
- Self-hosted deployments keep patient data entirely within your own infrastructure, simplifying HIPAA compliance
- A basic agent can be configured in minutes; full EHR integration takes a short setup period before go-live
The Real Cost of Traditional Healthcare Scheduling
The Structural Problem
Manual scheduling puts front-desk staff in a repetitive loop. A disproportionate share of their day goes to routine calls — new patient bookings, rescheduling requests, insurance questions — that offer no clinical value but can't be left unanswered. During peak morning hours, overflow is inevitable. After hours, patients hit voicemail.
A VHA study across 285 facilities measured what that looks like in practice: average call abandonment ran at 12%, and average speed of answer was 87 seconds — both well above the VHA's own performance targets of under 5% abandonment and under 30 seconds to answer. If a public health system with standardized protocols struggles to hit those numbers, smaller practices face similar or worse challenges with fewer resources.
The Patient Retention Consequence
Scheduling friction doesn't just delay care — it drives patients away. A 2022 vendor survey of over 1,000 patients found 61% had skipped a medical appointment in the past year because scheduling was too much hassle. A separate 2023 survey found 42% of patients would switch providers after being rescheduled twice.
These aren't hypothetical risks. Every unanswered call and every booking that requires a callback is a point where the patient relationship weakens — and that attrition eventually shows up in revenue.
The No-Show Revenue Gap
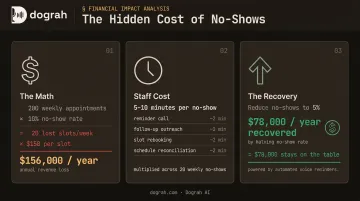
No-shows are the most measurable downstream consequence. The revenue math is direct: a practice running 200 appointments per week at a 10% no-show rate loses roughly 20 slots weekly. At an average visit value of $150, that's $156,000 in unrealized revenue per year — before accounting for staff time spent on reminder calls and rebooking. A reduction to 5% no-shows recovers half that figure without adding a single new patient.
- Staff time: Each no-show that requires manual outreach costs 5–10 minutes of front-desk time across reminder, follow-up, and rebooking
- Slot waste: Unfilled slots can't be recovered retroactively — the revenue loss is permanent
- Cascade effect: Chronic no-shows distort scheduling templates, leading to overbooking or under-utilization depending on how practices compensate
How Conversational AI for Healthcare Scheduling Works
Beyond IVRs and Keyword Matching
Traditional IVR systems are essentially phone menus with numeric inputs. A patient calling to book with a specific provider on a specific day can't do that through "press 1 for scheduling." They navigate menus, reach the wrong department, or abandon the call.
Conversational AI works differently. Using speech-to-text (STT) and large language model (LLM) reasoning, the system converts spoken patient requests into structured intent — then decides what to do next based on workflow logic and real-time data. A patient saying "I need to see Dr. Patel on a Tuesday afternoon" is understood contextually, not keyword-matched.
Platforms like Dograh AI go further with a custom STT dictionary that recognizes healthcare-specific terminology — clinician names, department acronyms, drug names — reducing recognition errors that would break the conversation. The LLM layer then handles intent detection and response logic, routing the call to the right scheduling branch: new patient intake, specialist referral, follow-up booking, or urgent triage.
The End-to-End Scheduling Workflow
Here's what a voice AI agent handles without human involvement:
- Patient calls inbound — agent greets the caller, identifies the purpose
- Context authentication — collects name, date of birth, and other verification fields
- Real-time availability check — queries the EHR or scheduling system via API
- Slot matching and confirmation — offers available times, confirms the booking
- EHR write-back — logs the confirmed appointment directly to the scheduling system
- Post-call follow-up — outbound reminder calls or messages at configurable intervals
EHR integration happens through standard APIs. The major platforms all expose what's needed:
- Epic — FHIR-based scheduling APIs for booking, rescheduling, and status updates
- Oracle Health — Millennium FHIR R4 Appointment resource
- athenahealth — appointment API supporting real-time read and write
Provider-specific rules, specialty routing, and pre-visit screening questions are handled through conditional workflow branches.
Latency and Conversational Quality
Patients disengage fast when an automated system hesitates — particularly on outbound calls, where the first few seconds determine whether the conversation continues.
Dograh AI's architecture targets sub-600ms end-to-end response times. The system also supports Speech-to-Speech (S2S) orchestration using models like Gemini Flash Live and OpenAI GPT-Realtime-2, which bypasses the STT-LLM-TTS handoff chain and reduces latency further, producing more fluid, natural-sounding conversations.

Multilingual Access
Healthcare serves diverse patient populations. Dograh AI supports 70+ languages natively with mid-call language switching — meaning a patient can shift languages mid-conversation without the call failing. The platform can be extended to hundreds of additional languages through third-party STT/TTS providers, and STT trained on healthcare terminology maintains accuracy across varied accents and clinical language.
For clinics in multilingual communities, this removes a real access barrier that staff-only phone lines can't solve without hiring for language coverage.
What Healthcare Providers Actually Gain
24/7 Coverage Without Added Headcount
Zocdoc's analysis of its own platform data found 37% of appointments were booked between 5 PM and 9 AM, with 17% on weekends. A practice that closes its phones at 5 PM is turning away more than a third of its potential scheduling volume.
Voice AI agents handle inbound calls at any hour with no hold queue and no overtime cost. Dograh AI's platform scales dynamically to match call volume — no configuration changes needed whether it's a weekday rush or a late Sunday evening.
No-Show Reduction Through Outbound Reminders
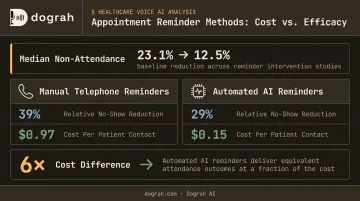
Automated outbound reminder calls are the most direct lever for reducing no-shows. A systematic review of 29 studies published in PMC found:
- Median baseline non-attendance rate: 23.1%
- Median rate after reminders: 12.5%
- Manual telephone reminders: 39% relative reduction in non-attendance
- Automated reminders: 29% relative reduction
The same review found automated reminder costs averaged €0.14 per patient contact (roughly $0.15) — compared to €0.90 ($0.97) for manual telephone reminders. That's a six-fold cost difference for a channel that still cuts no-show rates.
Dograh AI's outbound agent calls patients at configurable intervals before appointments, confirms attendance, offers rescheduling when a patient signals they can't come, and updates the EHR in real time — all without staff involvement.
Staff Reallocation to Higher-Value Work
When AI handles routine booking calls, front-desk staff have time for work that actually requires human judgment: prior authorizations, care coordination, in-person patient support, and complex scheduling involving multiple providers or insurance exceptions.
The ratio of AI-handled calls to staff-handled calls shifts — and the hours that remain go toward higher-leverage work that drives better patient outcomes.
Patient Experience and Loyalty
A 2023 JAMA Internal Medicine study found that when patients submitted questions to both physicians and AI chatbots, AI responses were preferred 78.6% of the time on quality and empathy metrics. That study focused on written Q&A rather than voice scheduling — but the data makes the point: patients don't automatically prefer human interaction when the alternative is better.
A well-configured voice agent that answers immediately, speaks clearly, and completes a booking in under two minutes will consistently outperform a rushed scheduler with six calls in queue.
Inbound and Outbound: Two Sides of AI Scheduling
Most practices think about AI scheduling as an inbound tool — handling new appointment requests, answering questions about location and insurance, routing urgent calls to clinical staff. That's accurate, and it's the highest-visibility use case.
Outbound is where the ROI concentrates.
Outbound AI scheduling use cases:
- Appointment reminders (configurable timing before visit)
- Confirmation calls after prior authorization clears
- Rescheduling outreach when a slot opens or a patient cancels
- Post-visit follow-up scheduling
Automated outbound reminders consistently cut no-show rates — the gap between a kept appointment and a missed one often comes down to whether a patient got a timely call. The key variable is voice quality. Outbound calls have roughly five seconds to establish credibility before a patient disengages or hangs up. A robotic-sounding automated call fails that test.
Dograh AI addresses this with a hybrid pre-recorded and TTS voice feature — mixing real human voice clips with TTS fallback in the same cloned voice. The result is an outbound call that sounds credibly human from the first word. Dograh AI's own outbound data shows 2× better conversion rates using this hybrid approach versus pure TTS — at up to 3× lower cost. For healthcare practices, that translates directly into fewer missed appointments and lower administrative overhead per confirmed visit.
Data Privacy, HIPAA, and the Case for Self-Hosted Voice AI
The Compliance Baseline
Any AI system that creates, receives, maintains, or transmits protected health information (PHI) is a business associate under HIPAA. That means a signed Business Associate Agreement (BAA) is required, and the vendor must meet Security Rule requirements: encrypted data in transit and at rest, audit controls, role-based access, and transmission security.
HHS's cloud computing guidance is explicit: a cloud service provider that maintains ePHI is a business associate even if it doesn't hold the encryption key. No structural workaround exists for cloud-hosted AI tools — that classification sticks regardless of how data is encrypted or routed.
The Vendor Compliance Overhead Problem
Every cloud-based AI scheduling vendor you evaluate adds procurement overhead. HIPAA BAA review, SOC 2 audit assessment, data processing agreements, security questionnaires — these processes take time, often weeks, and they repeat for each vendor added to the stack.
For healthcare organizations with limited IT and legal resources, this creates real friction between evaluation and go-live.
Self-Hosted Voice AI: The Architecture That Changes the Math
When a healthcare provider deploys voice AI within their own infrastructure (on-premise or private cloud), patient data never leaves their systems. Audio processing, STT, LLM inference, and TTS all run within the provider's controlled environment. Dograh AI doesn't touch the data.
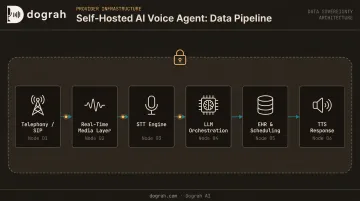
In Dograh AI's fully self-hosted model, the data flow looks like this:
- Telephony/SIP receives the call
- Audio streams into a self-hosted real-time media layer
- STT converts speech to text within the provider's environment
- LLM orchestration decides the next action
- Tool calls hit the provider's own EHR and scheduling systems
- TTS speaks the response back, entirely within the provider's infrastructure
The provider controls encryption keys (BYOK), audit trails, access controls, and retention policies for all STT, TTS, and LLM services. Dograh AI's open-source codebase (BSD 2-Clause license on GitHub) is fully auditable — no black-box components, no opaque vendor pipelines.
The practical compliance checklist for any AI scheduling platform:
- BAA availability confirmed in writing
- Data residency controls (can data be restricted to a specific geography or environment?)
- Encryption in transit (TLS 1.3) and at rest (AES-256)
- Role-based access control
- Complete audit logging of all interactions
- Self-hosting option if data sovereignty is a requirement
With a self-hosted Dograh AI deployment, every item on this checklist is satisfied within your own infrastructure. No vendor enters the HIPAA compliance chain, and procurement goes from weeks of review to a single internal sign-off.
Getting Started: Implementing Conversational AI in Your Practice
Map Your Highest-Volume Touchpoints First
Before selecting a platform, identify where scheduling volume is highest and most repetitive:
- New patient appointment booking
- Existing patient rescheduling
- Outbound reminder calls
- After-hours inbound requests
These are where AI delivers the fastest ROI and lowest implementation risk. They're also where unanswered calls have the most direct revenue impact.
Use a Phased Rollout
Dograh AI recommends starting with a single high-volume, predictable workflow — outbound appointment reminders are the recommended entry point for most healthcare organizations. Reminder calls have a clear success metric (no-show rate), are lower-risk than live inbound booking, and generate measurable ROI quickly.
A basic agent can be configured in Dograh AI's workflow builder in minutes using pre-built healthcare templates for appointment scheduling, reminders, triage routing, and after-hours handling.
Production readiness — meaning full EHR integration, scheduling rule customization, telephony configuration, and compliance validation — requires additional setup. Complexity scales with the EHR system, the number of providers and specialties involved, and whether self-hosted or cloud deployment is chosen.
Integration Questions That Drive Vendor Selection
Ask these before committing to any platform:
- Does it integrate directly with your EHR via standard APIs (FHIR, HL7)?
- Which telephony providers does it support — Twilio, Vonage, Telnyx, custom SIP trunks?
- Can scheduling rules be customized per specialty, provider, and location?
- Is self-hosting available if data sovereignty is a requirement?
- What does the BAA process look like — and how long does it take?
Dograh AI integrates with major telephony providers and uses webhook-based API connections to EHR and scheduling systems. For organizations with legacy telephony infrastructure, the platform supports custom SIP adapters — meaning older systems don't become a blocker during vendor selection.
Frequently Asked Questions
Frequently Asked Questions
Can you use AI for scheduling?
Yes. Modern conversational AI handles end-to-end appointment scheduling — booking, rescheduling, cancellations, and reminders — via voice and text. Platforms integrate directly with EHR and calendar systems through standard APIs, automating what previously required a staff member on every call.
Is conversational AI for healthcare scheduling HIPAA compliant?
AI scheduling tools can be made HIPAA compliant through encrypted data handling, audit logging, role-based access controls, and signed BAAs with vendors. Self-hosted deployments go further — patient data never leaves the provider's own infrastructure, removing third-party data processing risk entirely. Platforms like Dograh AI take this further with self-hosted OSS deployments — patient data stays entirely within the provider's own infrastructure, with no third-party processing risk.
How does conversational AI reduce patient no-shows?
Outbound AI agents call or message patients at configurable intervals before their appointment, prompting confirmation or rescheduling. Patients who can't attend are rescheduled immediately, and the EHR is updated in real time — closing calendar gaps before the appointment window arrives.
Can AI voice agents support multiple languages for diverse patient populations?
Leading platforms support 70+ languages with mid-call switching, so patients can speak naturally in their preferred language without the call failing. This directly serves non-English-speaking patients who are often left behind by staff-only phone lines.
Does AI scheduling replace front-desk staff?
No. AI handles tier-1 repetitive scheduling tasks — routine bookings, reminder calls, rescheduling requests — so staff can focus on prior authorizations, care coordination, complex patient situations, and in-person engagement. It's a staffing augmentation model, not a replacement.
How quickly can a healthcare practice deploy conversational AI for scheduling?
A basic agent can be configured in minutes using pre-built templates. Full production readiness — EHR integration, scheduling rules, telephony, and compliance validation — typically takes days to a few weeks, depending on EHR complexity and whether you're deploying to cloud or self-hosted infrastructure.