That distinction matters more than most healthcare IT teams realize when deciding where to deploy voice AI first. Get the sequencing wrong and you'll either automate the wrong problem or launch an outbound program without the compliance infrastructure to support it.
The pressure to act is real: the global AI voice agents in healthcare market was valued at $468M in 2024 and is forecast to reach $3.2B by 2030. Meanwhile, McKinsey research found that 60% of healthcare consumers hit barriers when scheduling with their preferred provider — and 27% simply went elsewhere rather than wait.
This post covers what inbound and outbound AI voice agents actually do in healthcare, how they compare across key dimensions, and a practical framework for deciding which to prioritize.
Key Takeaways
- Inbound agents handle patient-initiated calls (scheduling, billing, prescription refills) through natural conversation that resolves calls end-to-end — no rigid IVR menus.
- Outbound agents proactively reach patients at scale — post-discharge follow-ups, appointment reminders, chronic care check-ins — without adding headcount.
- Inbound is the higher-ROI starting point for most organizations because workflows are predictable and containment rate is immediately measurable.
- Outbound requires upfront compliance work: TCPA consent management, answering machine detection, and call timing rules all need to be in place before launch.
- Data sovereignty matters in both directions: self-hosted or private cloud deployments keep PHI inside your own infrastructure, cutting out the vendor BAA chain.
Inbound vs. Outbound: Quick Comparison
Here's how inbound and outbound voice AI compare across the dimensions that matter most in healthcare deployments:
| Dimension | Inbound | Outbound |
|---|---|---|
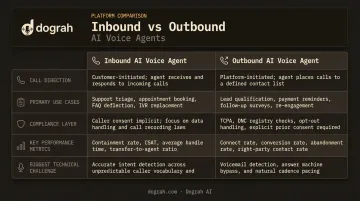
| Call direction | Patient calls the provider | Agent dials the patient |
| Primary use cases | Scheduling, prescription refills, billing, triage routing | Post-discharge follow-up, reminders, chronic care check-ins, preventive outreach |
| Compliance layer | HIPAA PHI handling, patient authentication, EHR read/write | All inbound requirements + TCPA consent, AMD, call timing windows, voicemail handling |
| Key performance metric | Containment rate, average handle time | Answer rate, completion rate, readmission/no-show reduction |
| Biggest technical challenge | Medical vocabulary accuracy, multi-turn intent handling | First-15-second engagement, AMD accuracy, establishing legitimacy quickly |
What Are Inbound AI Voice Agents in Healthcare?
Inbound AI voice agents receive patient-initiated calls and handle them conversationally using ASR (automatic speech recognition), NLU (natural language understanding), and TTS (text-to-speech). The key difference from a traditional IVR system: the patient speaks naturally, the agent understands intent, and the task gets completed — no menu trees, no hold music, no callbacks.
Healthcare front desks are under sustained staffing pressure — MGMA reported 40% front-office turnover in 2022. Inbound voice AI absorbs call volume without proportional headcount, serves patients outside office hours, and frees staff for interactions that require human judgment.
What Separates a Capable Inbound Agent from a Phone Menu
Real-time EHR integration is the dividing line. An agent that can't read schedule availability, verify patient identity, or write a confirmed appointment back to Epic or Cerner is still a phone menu — just a more expensive one.
Beyond integration depth, healthcare-specific inbound agents require:
- Custom vocabulary layers for medication names, ICD codes, insurance identifiers, and clinical shorthand that generic STT models routinely mangle
- Patient authentication workflows — verifying name, date of birth, callback number, or member ID before any PHI is accessed
- HIPAA-compliant data handling at every layer of the call stack, including the ASR, LLM, and TTS components
Platforms like Dograh AI handle this through a custom keyword dictionary feature that preserves terms like "HbA1c" or "OPD" intact, combined with configurable patient verification nodes that can retry on mismatch and escalate to staff on repeated failure.
Inbound Use Cases
Most health systems see the clearest, fastest ROI from four use cases:
Appointment scheduling and management — the highest call volume in most health systems. The agent verifies identity, checks EHR availability, books or reschedules, and sends a confirmation. Workflows are well-defined and ROI is measurable within weeks, making this the right pilot starting point.
Prescription refill requests — the agent verifies patient identity and medication eligibility, transmits the request to the pharmacy, and confirms. A workflow that used to require multiple callbacks closes in a single call.
Billing and insurance inquiries — inbound agents can explain charges, verify coverage status, and set up payment plans, routing genuinely complex disputes to a human specialist rather than queuing every billing call. Note: TCPA rules exclude billing and financial content from healthcare exemptions, so this use case is inbound-only.
Clinical triage routing — captures symptom information and urgency level, then routes callers to an ED, urgent care, telehealth queue, or nurse callback. Accuracy here is non-negotiable. Emergency intent detection — chest pain, stroke symptoms — should trigger mandatory escalation protocols with no exceptions.
What Are Outbound AI Voice Agents in Healthcare?
Outbound healthcare voice agents initiate calls to patients on behalf of the provider. Not to sell anything — to follow up, remind, check in, and close care gaps at a scale no human team can replicate.
The technical challenge is immediate: unlike inbound calls where the patient already wants something, outbound agents must establish context and legitimacy within the first 15 seconds. A patient who doesn't recognize the number will hang up or dismiss the call as spam. Pacing, natural interruption handling, and voice quality all matter more on outbound than inbound.
The Compliance Layer Outbound Teams Often Underestimate
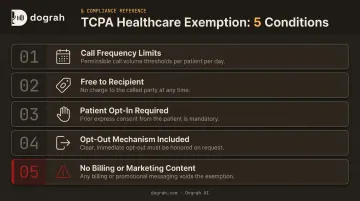
TCPA governs outbound automated calls, and the healthcare exemption is narrower than most teams assume. FCC rules allow non-telemarketing healthcare calls — appointment reminders, post-discharge follow-up, prescription notifications, lab results — but with strict conditions:
- Maximum 1 message per day, up to 3 calls or texts per week per provider
- Calls must be free to the recipient
- Patients must have opted in (provided their number to the provider)
- Must include opt-out mechanisms (keypress or toll-free number)
- Billing, financial, and marketing content voids the exemption entirely
Answering machine detection (AMD) is equally critical. Leaving a voicemail that includes PHI — a medication name, a diagnosis, a discharge date — creates a compliance breach. Outbound deployments need AMD configured before launch, with PHI-safe voicemail behavior defined.
Hybrid Voice for the Trust Window
Dograh AI's hybrid pre-recorded + TTS feature is well-suited for outbound healthcare calls. A hospital can record an actual clinician's voice for the opening of a post-discharge call — "Hello, this is a follow-up call from [hospital name]" — and then fall back to TTS for dynamic content like medication names, appointment dates, or patient-specific instructions. The voice remains consistent throughout because the TTS fallback uses the same cloned voice.
This matters because the first few seconds determine whether a patient stays on the line. The hybrid approach delivers 2x better conversions and costs up to 3x less than pure TTS outbound — a meaningful difference at high call volumes.
Outbound Use Cases
- Post-discharge follow-up: A 2025 JAMA Network Open meta-analysis found outpatient follow-up within 30 days cuts 30-day readmission risk by 32%. With average readmissions costing $16,300 and CMS HRRP penalties reaching 3% of Medicare payments, proactive follow-up has a direct financial case.
- Appointment reminders with rescheduling: No-show rates run from 12% to 42% in outpatient settings. Automated phone reminders reduced no-shows from 17.5% to 13.1% in one documented study — straightforward revenue protection.
- Chronic care and medication adherence check-ins: 41% of adults with hypertension are nonadherent to their medications (CDC). Regular outbound check-ins for patients with diabetes, hypertension, or similar conditions scale what would otherwise demand significant nursing time.
- Preventive care and screening outreach: Population health programs can remind at-risk patients about annual screenings, vaccinations, or overdue preventive visits — without adding headcount proportionally.
Which Should Healthcare Organizations Prioritize?
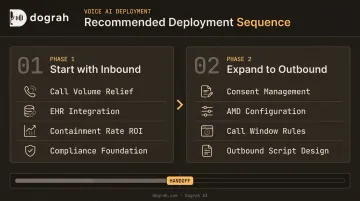
This isn't an either/or decision long-term. But most organizations should sequence deployments deliberately rather than attempt both simultaneously.
Choose Inbound First If:
- Your primary pain is call volume, hold times, and front-desk staffing
- Administrative backlogs are causing patient access friction
- You need fast, measurable ROI to justify the broader voice AI investment
- Your EHR integrations and compliance infrastructure are still being built out
Inbound delivers faster ROI because the structure is predictable — the patient initiates with a specific task, the workflow is defined, and containment rate gives immediate proof of impact. A health system handling thousands of scheduling calls weekly can demonstrate ROI within weeks of deployment.
Choose Outbound First If:
- Readmission penalties are a material financial risk
- No-show rates are measurably impacting revenue
- A chronic care or population health program needs scale that current staffing can't provide
- Consent management and compliance infrastructure are already in place
Outbound requires more preparation before the first call goes out. Consent documentation, AMD configuration, call window compliance, and opening script design all need to be resolved upfront. For most organizations, the sequence is clear: build inbound foundations first, stabilize EHR integrations, then expand to outbound once compliance infrastructure is in place.
Data Sovereignty and HIPAA in Both Directions
HIPAA compliance is architectural, not a feature checkbox. The question isn't just "does the vendor sign a BAA?" — it's where PHI actually travels. Every vendor in the call path that touches patient data (ASR, LLM, TTS, telephony, analytics) must be covered by a BAA under HHS guidance.
For organizations operating across multiple regulatory jurisdictions, that vendor chain gets expensive fast. GDPR regions, state-level privacy laws, and strict data residency requirements each add procurement overhead and audit complexity.
Self-hosted or fully managed private cloud deployments eliminate this problem at the architectural level. Dograh AI supports fully air-gapped deployments where PHI never leaves the organization's own infrastructure, including locally hosted models like Whisper (STT), Kokoro (TTS), and Llama (LLM). That means:
- No HIPAA BAA negotiations with each subprocessor
- Voice data, transcripts, and call metadata stay within your VPC or data center
- Complete audit trails you own and control
Conclusion
Inbound and outbound AI voice agents in healthcare are complementary. Inbound handles the call volume problem. Outbound handles the patient outcomes problem. The sequencing question (which to deploy first) should be driven by the organization's highest-cost pain point today.
Whatever use case you start with, the platform choice matters as much as the use case itself. Prioritize data control, low-latency conversational quality, and EHR integration depth over feature lists. For healthcare specifically, self-hosted or private-cloud deployments remove HIPAA vendor processing overhead entirely, which matters at procurement time and at scale. Platforms like Dograh AI are built around those constraints from the ground up, rather than bolting compliance onto a general-purpose system.
The organizations that deploy thoughtfully, starting with one direction and building toward both, end up with infrastructure that compounds. Those that chase feature lists end up re-platforming 12 months in.
Frequently Asked Questions
What is a voice calling AI agent for healthcare?
A healthcare voice AI agent handles patient phone calls using speech recognition, natural language understanding, and text-to-speech — managing scheduling, billing, and post-discharge follow-up through natural conversation rather than rigid IVR menus. Unlike a basic phone bot, it completes transactions end-to-end and integrates directly with EHR systems.
What are AI voice agents used for in healthcare?
The two primary deployment modes are inbound (appointment scheduling, prescription refills, billing inquiries, triage routing) and outbound (post-discharge follow-up, appointment reminders, chronic care check-ins, preventive outreach). The highest-volume starting points for most organizations are scheduling on the inbound side and appointment reminders on the outbound side.
What is the difference between voice AI and IVR?
IVR forces callers through numbered menus and scripted prompts — press 1 for scheduling, press 2 for billing. Voice AI understands natural speech, handles multi-turn conversation, and completes tasks without requiring the caller to memorize menu options or repeat information across transfers.
Are AI voice agents HIPAA compliant?
HIPAA compliance is architectural, not a feature checkbox. Every vendor in the call path — ASR, LLM, TTS, telephony — must hold a signed BAA, and self-hosted deployments can keep PHI entirely within your own infrastructure. A vendor claiming "HIPAA compliance" without detailing their subprocessor chain isn't giving you the full picture.
What are the regulations for AI in healthcare?
HIPAA requires BAAs with every vendor processing patient data; TCPA governs outbound calling consent, frequency, and content restrictions. State privacy laws layer on additional requirements by jurisdiction. Administrative voice agents — scheduling, reminders, billing — typically fall outside FDA scope, which targets clinical decision-support AI.
Are AI voice assistants always listening?
Healthcare voice AI agents activate only on an incoming or outgoing call event — they do not passively monitor ambient audio. Data retention policies covering how long recordings or transcripts are stored and where are configurable and should be confirmed with any vendor before deployment.